INDICATIONS/CONTRAINDICATIONS
Colon interposition is performed most frequently when the stomach is not suitable or available for use as an esophageal substitute. Possible reasons include previous gastrectomy, tumor involvement of the stomach, and synchronous gastric cancer. The general indications for esophagectomy are similar to those described elsewhere in this text, and include esophageal cancer, end-stage motility disorders, and stenoses that have not responded to other treatments, and corrosive injury or trauma to the esophagus. The surgeon’s preferences, the presence of nonmalignant disease, and whether a vagal- sparing approach is being considered may also play a role in the decision to perform colon interposition.3 Colon interposition is also indicated as a salvage operation necessitated by failure of a previous esophageal substitute.
Mild diverticular disease is generally not a contraindication to the use of colon as an esophageal replacement, though extensive diverticulosis, frank diverticulitis, or inflammatory fibrosis may be. Similarly, the presence of a few colonic polyps, whether hyperplastic or adenomatous, that can be removed before surgery does not preclude colon interposition. The presence of extensive polyposis or malignancy, however, is an absolute contraindication.
 PREOPERATIVE PLANNING
PREOPERATIVE PLANNING
An assessment of the patient’s cardiopulmonary reserve is essential prior to any major surgical undertaking such as esophagectomy. A thorough history should be obtained, focusing on respiratory difficulties at rest or with exertion, exercise tolerance, chest pain, or fatigability. In addition, any symptoms suggestive of possible colonic pathology, such as diarrhea or constipation, or a history of inflammatory bowel disease, diverticular disease, colonic neoplasia, prior colon resection, or abdominal aortic disease should be elicited.
Physical examination should concentrate on cardiopulmonary findings. When questions arise about coexistent cardiac or pulmonary disease based on the patient’s age, comorbidities, physical signs or symptoms, formal physiologic testing should be pursued. Pulmonary function testing, including expiratory flows, lung volumes and diffusion capacity, can objectify the severity of concomitant obstructive or restrictive lung disease. Lung function should be optimized through smoking cessation, bronchodilators, expectorants, antibiotics, and pulmonary rehabilitation, as necessary. Cardiac imaging and stress testing can elicit subtle changes in cardiac function suggestive of ischemia, cardiomyopathy, or valvular heart disease. When coronary artery or valvular pathology is deemed significant, interventions such as angioplasty, coronary stenting, or even open heart surgery should be completed prior to elective esophageal surgery in an effort to minimize perioperative risk at the time of esophagectomy.
One advantage of esophagectomy in the setting of benign disease compared to malignancy is that surgery can often be delayed pending optimization of cardiopulmonary issues, nutrition, or other comorbidities. While the patient and treating physicians may feel a time pressure to treat an esophageal malignancy, end-stage benign esophageal disorders tend to be fairly long-standing problems that can be temporized while a thorough work-up is completed and risk factors addressed. Enteral or parenteral support may be pursued if a patient is unable to tolerate an adequate oral diet. While no absolute thresholds exist for abandoning surgery due to pulmonary or cardiac compromise, such objective information can often influence the surgeon in making a decision for or against esophageal reconstruction and in the type of operation chosen.
When the colon is being considered as a potential esophageal substitute, colonoscopy should be performed to evaluate the status of the colonic mucosa. Colonoscopy is preferred to an air contrast barium enema because mucosal detail is better assessed and polyps or masses can be biopsied or resected.
As the colon should be adequately prepared for colonoscopy as well as for subsequent surgery, the colonoscopy may be scheduled a day or two before foregut reconstruction to allow both procedures following a single bowel prep. Our preferred regimen is to admit the patient to the hospital 2 days before surgery for bowel prep, consisting of 4 L of GoLYTELY (polyethylene glycol electrolyte solution; Braintree Laboratories Inc., Braintree, Massachusetts) administered orally, followed by colonoscopy the day before surgery along with oral neomycin and metronidazole.
Controversy exists regarding the necessity of routine preoperative mesenteric arteriography when colonic interposition is planned. As the successful use of colon is dependent upon an adequate vasculature, the surgeon should have a low threshold to perform such studies. When arteriography is performed, selective injections of the celiac artery, superior mesenteric artery (SMA) and inferior mesenteric artery (IMA) should be undertaken, including lateral views, and paying particular attention to any anatomic aberrancy. When the left colon is to be utilized for interposition, the most important angiographic finding is the status of the IMA, particularly at its origin, which can be stenosed in elderly individuals or in those with peripheral vascular disease. As the blood supply of a left colon interposition critically depends upon adequate inflow from the IMA, a significant stenosis of this vessel is a contraindication to the use of the left colon for esophageal reconstruction.4 A right colon interposition, based on the middle colic branches of the SMA, can be used in this situation, as it is not dependent upon IMA inflow. Other angiographic features thought important to the successful use of left colon for interposition include a visible ascending branch of the left colic artery, a well-defined anastomosis between the left colic and middle colic systems (along the marginal artery of Drummond), and a single middle colic trunk prior to division into right and left branches. Because of its more reliable and predictable arterial inflow and venous outflow, not to mention its better size match to the native esophagus, the left colon is generally preferred over the right colon for esophageal replacement.
As patients undergoing foregut reconstruction frequently have undergone multiple prior abdominal operations, mesenteric arteriography can help to define the resultant vascular anatomy and ascertain that vessels supplying planned esophageal substitutes are patent. In particular, prior operations involving the greater curvature of the stomach may have disrupted the right gastroepiploic artery, critical to the blood supply of a gastric pull-up, or the middle colic artery and marginal artery of Drummond, critical to the blood supply of a colon interposition. Preoperative knowledge of such vascular abnormalities can help the surgeon navigate the operation and save considerable time and effort during the procedure.
 SURGERY
SURGERY
Choosing Short-segment or Long-segment Colon Interposition
Given the ability of the colon to reach either into the thorax or all of the way to the neck, colonic interposition may be undertaken after resection of either short or long segments of the esophagus. While the surgeon may want to preserve as much normally functioning esophagus as possible for certain indications, such as a nondilatable esophageal stricture, resecting only a limited distal segment carries several concerns about subsequent reconstruction. The esophageal anastomosis, whether it is to stomach, small intestine, or colon, frequently must be intrathoracic in location after a limited distal esophagectomy. Only if there is sufficient length of abdominal esophagus can the subsequent anastomosis be placed in the abdominal compartment.
Three potential problems relate to placement of the anastomosis within the thorax. First, a thoracotomy or thoracoabdominal incision is generally necessary and is associated with significant pain, a poor cosmetic or functional outcome, and the necessity for single-lung ventilation during surgery, as well as the additional operative time necessary to open and close the incision and reposition the patient. While a transhiatal stapled anastomosis using a circular stapling device, or a thoracoscopic esophageal mobilization and anastomosis may obviate the need for a large thoracic incision, such techniques may not be feasible, especially in the setting of a reoperative procedure.
The second potential problem is that the consequences of an intrathoracic leak may be more devastating than those resulting from a leak in the neck. Multiple surgical series have reported higher morbidity and mortality associated with intrathoracic esophageal leaks, leading to mediastinitis, empyema and systemic sepsis, although these risks may be decreasing in recent years.5 Relative to near-total esophagectomy with a cervical anastomosis, which can often be completed without a thoracic incision and places the anastomosis near the thoracic inlet, resection of a limited segment of the distal esophagus carries with it the potential morbidity of both the thoracic incision and the intrathoracic anastomosis.
The third potential problem is reflux through the short colonic conduit, leading to esophageal mucosal injury or heartburn. Anastomoses high in the chest or in the neck appear to be less prone to subsequent reflux, though the length of the interposed conduit may be an important determinant of the volume of refluxate as well.
In general, we avoid short-segment colonic interpositions and prefer near-total esophagectomy with a cervical esophagocolonic anastomosis whenever possible. If the length of colon available for interposition is a concern, an intrathoracic anastomosis is preferably made high in the chest to minimize postoperative reflux.
Colon Conduit Preparation in Foregut Replacement
Both left and right colon interposition techniques have been described. In general, the left colon is preferred because of the better predictability of its blood supply and the better size match to the remnant esophagus. A successful outcome following colonic interposition requires close teamwork between the surgeon and the anesthesiologist. The maintenance of adequate mesenteric perfusion is critical to prevent ischemia of the conduit. Vasopressors should be avoided and adequate blood pressure provided through the use of intravenous fluid replacement and blood products, as indicated. This plan should be clearly communicated and discussed with the anesthesia team prior to induction of general anesthesia, as well as with any new staff substituted throughout what is often a prolonged procedure.
When the vagus nerves have been resected as part of an esophagectomy and colon interposition is planned, the proximal three quarters of the stomach should be removed to avoid problems with delayed gastric emptying that can result when the denervated stomach is left intact. Typically the colon is anastomosed distally to the gastric antrum, and a pyloric drainage procedure is added. If a vagal-sparing esophagectomy is performed, the whole stomach may be left intact and gastric drainage avoided.
Left Colon Interposition
The term “left colon interposition” is a misnomer in that it refers to interposition of the transverse colon, not the left colon. The name is derived from the fact that its blood supply is based off of the ascending left colic artery, a branch of the IMA, and the left colic vein, a tributary of the inferior mesenteric vein (IMV). The blood supply to the conduit is dependent upon communication between these vessels and the marginal arteries and veins originating from the middle colic circulation, the origins of which get divided as part of the procedure (Fig. 28.1).
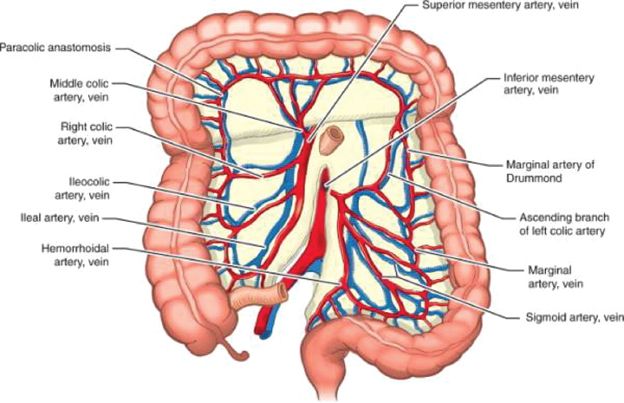
Figure 28.1 Vascular anatomy of the colon.
The operation is performed through an upper midline laparotomy incision and commences by dissection and vascular isolation of the colon conduit prior to resection of the esophagus and stomach. This sequence is chosen to allow for adequate time to assess the perfusion of the prepared colon conduit before committing to its use. The descending colon is mobilized laterally along the white line of Toldt from the splenic flexure to the beginning of the sigmoid colon, as for a colectomy. Care should be taken to prevent disruption of the colonic mesentery as well as to avoid the left ureter. The ascending branch of the left colic artery is assessed by direct palpation. The right colon is then mobilized in a similar fashion. The greater omentum is dissected from the transverse colon, preserving the transverse mesocolon. The base of the left and transverse mesocolon is next freed from the retroperitoneum, preventing inadvertent division of the IMV in the region of the ligament of Treitz.
The middle colic artery and vein are identified by transillumination of the transverse mesocolon and by direct palpation, then dissected near their origins from the superior mesenteric artery and vein, respectively. This part of the operation is one of the most challenging and important. It is critical to divide these vessels as near their origins as possible, in order to preserve communications between the right and left branches of the middle colic artery (as well as branches of the middle colic veins) and any vascular arcades within the transverse mesocolon. Once these vessels have been dissected, they are occluded with bulldog vascular clamps to allow assessment of colon perfusion while the operation is progressing and prior to the irreversible step of vessel transection.
The region of the distal transverse colon is then grasped and retracted cephalad, demonstrating the tether point of the ascending left colic vessels (Fig. 28.2). This portion of the colon typically reaches the level of the xiphoid process and is marked with a suture along the antimesenteric border. Using an umbilical tape, the distance between the xiphoid and the planned proximal anastomosis (typically within the left neck) is measured, adding several additional centimeters of length to assure an adequate reach. The umbilical tape is cut to this length and used to measure the distance proximally along the colon from the suture on the distal transverse colon, usually reaching a point at approximately the mid-ascending colon. The colon is marked with a second suture at this point to denote the location for subsequent bowel division, defining what will become the proximal end of the isoperistaltic colon conduit. Vascular contributions to the colon conduit from the right colic and ileocolic vessels residing within the right mesocolon are dissected and occluded with bulldog vascular clamps, as they will need to be divided subsequently to allow interposition.
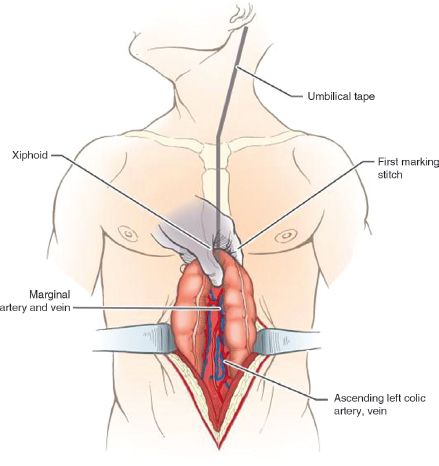
Figure 28.2 The colon is retracted cephalad to note the tether point of the ascending left colic vessels. This point typically reaches the xiphoid process and is marked with a suture along the antimesenteric border. The distance between this point (or xiphoid) and the cervical esophageal remnant is measured with an umbilical tape, adding a few additional centimeters of length.



